Training Cross-Disciplinary Innovators
Sanjit Misra, M.B.A.
Duke University, Fuqua School of Business
Introduction
The rapid growth of costs in the CV space due to the aging population highlights the need for innovation to ensure the sustainability of our health care ecosystem. One way to address this need is through leveraging previously siloed disciplines to bring them together to address some of the most pressing concerns in CV in the hopes of driving cost and clinical efficiencies.
Much of the innovation of the past has focused on creating new therapies, drugs, procedures and medical devices. Although they have yielded exceptional results, these advances are highly niched innovations in particular spaces where the focus needs to be more holistic and disruptive.1 To promote more disruptive innovation in health care, multiple disciplines need to come together to bring thoughtful and groundbreaking innovations to fruition.
This process requires significant time and resources, which, particularly for physicians, are not inherently available. Programs such as the Harvard Medical School Center for Primary Care’s Abundance Agents of Change (AoC) program to promote interdisciplinary innovation highlights the resources needed to effect this change. This program offered $20,000 to interprofessional student teams that address a primary-care need identified by community health centers 2
Beyond these programs, many physician-led groups are establishing online resources to enable cross-disciplinary innovation. For instance, the American Medical Association created the Physician Innovation Network to enable physicians to connect with technology companies and entrepreneurs to collaborate on new digital health tools.3 Many universities are also hosting events to promote the idea of cross-disciplinary collaboration in health care. NYU hosted its first-ever “Healthcare Makerthon“ to attract disparate skill sets to enable collaboration to bring ideas to market.4 However, as medicine continues to evolve, physicians must carve out time to leverage these available resources to develop the solutions of the future.
Cross-disciplinary collaboration has become an essential part of innovation in all parts of science. It is viewed as key to solving issues on a global scale, because it recognizes the synergistic and skill-combining benefits of multiple fields. For example, Dr. Bora Chang, a physician from Duke, launched kelaHealth, a company based on machine learning on millions of surgical patient data points. She was able to stratify complication risks for surgeries across many service lines (e.g., cardiology, GI) with not only the support of the Duke Department of Surgery, but also the Department of Statistics and Computer Science. This support allowed her to obtain initial funding and eventually spin the company out of Duke to work with other health systems and surgical vendors.5 Similar stories are found across the health care spectrum, from oncology, where issues revolve around data aggregation, to primary care. For instance, companies such as Heal leverage physician and technology leaders’ knowledge to change the way primary care is delivered, by providing on-demand concierge care at prices below many urgent care clinics. To continue these innovations, incentives need to be aligned to drive these entrepreneurs toward these types of partnerships and innovations.
The sponsors of these programs are often large institutions that have the resources to implement programs that require vastly different skill sets. For instance, in addition to the programs backed by large academic institutions discussed in this paper, the University of Louisville opened the Cardiovascular Innovation Institute (CII) as a joint initiative with Jewish Hospital and St. Mary’s Health care in 2007 to focus on discovery, R&D and implementation of innovations in CV treatment. The goal of CII was to create a multidisciplinary institute focused on propelling ideas from research to implementation at a rapid pace by bringing together previously disparate disciplines under one roof.6 Similar programs continue to pop up throughout the country. The sponsors are large academic institutions or consortiums, often backed by grants or corporate sponsors. T University of Michigan’s Medicine Department is another example. It launched its Multidisciplinary Cardiovascular Research Training program that aims to bring basic and clinical sciences together for the purpose of studying cardiovascular disease.7
Beyond academic institutions, many other innovative programs encourage the cross-training of leaders. For instance, the American Heart Association established the Center for Health Technology & Innovation (CHTI). Its purpose is similar to that of many academic institutions, though less formally — to establish a consortium of strategic collaborations that link providers, entrepreneurs, researchers and patients, with the goal of building innovative and scalable solutions across the continuum of care.8 Similarly, other large groups, such as the American Medical Association, have built consortiums to formalize these linkages across the traditional and nontraditional stakeholders in health care. For example, the AMA partnered with Health2047 Inc., giving $27 million in funding, to help it invest in solutions that will fundamentally transform the health care ecosystem. Health2047 deploys its executives and advisers to provide expertise in medicin artificial intelligence, machine learning and network infrastructure, while leveraging the AMA’s network of physicians. 9
Many other programs similar to the collaboration between the AMA and Health2047 exist in the U.S. to encourage cross-disciplinary innovation in medicine. For example, Healthbox, a health care accelerator, makes small investments up to $100,000, and large investments with Intermountain’s $35 million Healthcare Innovation Fund, but combines these investments with consulting services to enable innovators to gain the multidisciplinary expertise needed to launch impactful companies. In fact, to provide more resources, Healthbox is now part of HIMSS, similar to the partnership between Health2047 and the AMA.10 Other examples include MATTER, a health care accelerator in Chicago that provides many of the same connections but also provides a layer of formal executive education to cross-train innovators in user-centered product design and development.11 Although some of these health care accelerators such as MATTER are standalone entities without formalized partnerships, they are in the minority. Accelerators such as Healthbox, Health2047 and Techstars have formalized relationships with large institutions, HIMSS, AMA and Cedar-Sinai, respectively, for the purposes of knowledge sharing, beta testing and cross-training.
Finally, although many of these accelerators focus on health care as a whole, many started out in more concentrated niches. For instance, Synecor, a health care accelerator in Chapel Hill, North Carolina, initially focused on interventional cardiology, with its internal expertise being in that space, while partnering with corporate leaders in the medical-device space. Synecor eventually opened up to all specialties to enable the creation of new disruptive medical-device technologies across the health care spectrum. It achieved this success by employing scientists who are inventors as well as savvy business leaders who could provide innovative ideas to portfolio companies. Moreover, Synecor established clinical and financial partnerships with leading organizations such as Stanford, Duke, Johnson & Johnson, Medtronic and Abbott that enabled Synecor to connect companies to the expertise required to drive innovation. Partnerships and internal expertise helped drive the accelerator’s successes, such as TransEnterix’s new laparoscopic surgical platform being recognized as “Innovation of the Year“ by the Society of Laparoendoscopic Surgeons to Aegis, closing a $5.1 million Series A round.12
These accelerators, consortiums, grants and more highlight the complexity and resources needed to launch programs to support the scalability and ideation of innovative solutions in health care. At the core, these programs aim to solve a misalignment of incentives between all these stakeholders to bring them together to focus on a common goal. This misalignment causes a lack of collaboration that can only be remedied by unified groups that focus on gathering all the groups to the table: physicians, engineers, statisticians, business leaders and more.13 Starting and sustaining models such as these is challenging but highly rewarding; we will explore one of the most successful versions through the Stanford Byers Center for Biodesign.
Stanford Byers Center for Biodesign
History
Biodesign was founded in August 2000 as part of the existing Stanford Bio-X program as a collaboration between the schools of medicine and engineering. In November 2000, Stanford Biodesign secured two sponsors in Johnson & Johnson and Guidant (now known as Abbott), which continue to be funders as of this report. These partnerships were established to obtain additional expertise that could be leveraged through the Biodesign program, particularly in the Innovation Fellowship. The program was set up to operate a multidisciplinary hub where fellows could tap into resources and infrastructure in business, medicine, design and engineering at Stanford.
The first cohort of the year-long Innovation Fellowship entered the program in September 2001. During that year, the Biodesign program focused on continuing to build the mentor network for the fellows. To further aid the fellows, the Biodesign Innovation Course was launched in September 2002 as a graduate-level course for engineering, medical and business students, in which student projects were focused on the needs of the fellows. Biodesign further taught a condensed version of the Biodesign process to interested participants and provided another layer of support for the fellows to succeed.
A key element of the program was the ability to bring in leaders from other parts of the industry to help these fellows connect with and understand the process beyond just the invention. The first “Emerging Entrepreneurs“ three-day workshop in 2005 is an example of this effort. Venture capitalists, MedTech entrepreneurs and other industry leaders attended and offered insight into how to start and run a company. Such insight was key in helping these innovators make their ideas a reality.
In addition to these connections, which are invaluable in creating and sustaining innovation, the Biodesign program worked to provide capital. In fact, in March 2006, the Stanford Coulter Translational Program was launched, supported by a $20 million sustaining endowment that allowed for six to eight Coulter grants every year for new medical technologies created by Stanford faculty. This capital allowed for easier access to funds to help launch ideas out of Stanford.
As the program continued to expand and grow, the diversity of expertise in the Biodesign teams led to potential challenges between the collaborating individuals. As a result, Biodesign hired Julian Gorodsky as the fellowship’s first psychologist, to address interdisciplinary team issues.
To continue the goal of disseminating the ideas of Stanford Biodesign, Stanford faculty (Zenios, Makower, Yock) and a GSB research associate, Lyn Denend, wrote their first textbook, titled “Biodesign: The Process of Innovating Medical Technologies,“ which sold 10,000 copies worldwide in August 2009. This effort was accompanied by an open-source website, eBiodesign.org, to enable easier access to the tools and processes developed.
With Biodesign’s growing influence, specifically in MedTech, the group published a series of web interviews of regulatory experts in February 2011 that covered a range of topics from the start to the end of the regulatory process to help innovators get their innovations through FDA approval. The series highlighted the importance of leveraging expertise outside the competencies of an innovation’s core team to bring the idea to fruition. The Biodesign program expanded on these efforts by formalizing a partnership with the FDA. These partnerships and others continued to enable alumni successes such as iRhythm in the U.S. (2006) and Consure Medical in India (2012).
Over time, the mission has remained unchanged, with continuing global partnerships, such as those forged with Japan in 2015, and ensuring the sustainability of these programs abroad via resourcing and funding. In 2016, Stanford Biodesign was rebranded as the Stanford Byers Center for Biodesign, consolidating finance and administration for the sake of streamlining.14
Philosophy
The Stanford Byers Center for Biodesign has been focused on enabling the most promising health-technology innovators by supporting them with the tools and processes delivered through mentors, coursework, industry leaders and more. The program is purposefully designed to cater to future innovators from a variety of backgrounds, including medicine, biosciences, engineering, computer science, product design, law and business. The program brings together this expertise to find solutions to unmet needs. Beyond the selection process, it sets students and fellows on a path for success by providing them access to Stanford’s schools of medicine, business, design and engineering as well as 200-plus industry leaders in the area. The program requires its innovators to be agile and to think outside their comfort zones.15
The process of innovation in the Biodesign program is one that has been taught at Stanford and around the globe since 2000. The idea is that this process can be taught and utilized for a wide range of applications in the health-technology field across a variety of expertise.
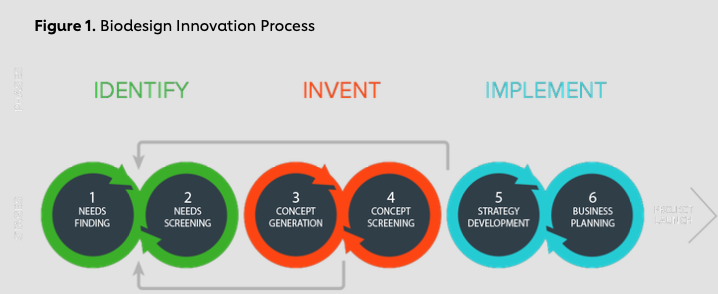
This process is broken down into three steps — Identify, Invent and Implement — that are taught to students, faculty and fellows. The most important step in this process revolves around Identify. It is a highly iterative process whereby trainees follow the full cycle of care to identify important unmet needs. They ask pointed questions to understand how each step affects all the stakeholders in the continuum of care. This process is key to remaining objective while surveying the hundreds of unmet needs and then narrowing them down to the ones that have the most potential to improve care and/or save the system money. The goal of this part of the process is to find two toro three promising ideas that can have a large impact.
The second step, Invent, requires a variety of skill sets pertaining to more than just medicine. This step requires rapidly testing hundreds of potential solutions to the problems in order to find better solutions. However, once good solutions present themselves, they need to be tested in terms of reimbursement and regulatory approvals as well as potential intellectual property- rights issues. Thus, the Biodesign program is a collaboration of stakeholders including physicians, engineers, business leaders and many more. It allows stakeholders to be cross- trained, learning nuances they would not have otherwise known. The goal is that this rapid prototyping leads to a viable, implementable solution.
The final phase of this process concerns Implementation, whereby trainees take their ideas to the next step by formulating deeper business plans that incorporate all of the above as well as options for funding and market potential. The Biodesign program supports these trainees by providing mentorship via industry leaders and other alumni to aid them in this final step. This iterative process exposes the trainees to the full cycle of developing a solution to a major problem from beginning to end. This level of cross-disciplinary training enables the trainees to continue their work as innovators even without the resources of Biodesign fully supporting them day in and day out.16
Use cases
The Biodesign program was created to realize synergies between physicians who live in the trenches and engineers who understand the available technologies. The intent was to bring a fresh perspective to large health care problems. The hope was that these often-disparate groups can come together to find novel solutions to difficult challenges that plague health care.17
One of the most successful companies to come out of the Biodesign program was iRhythm, which was founded by Dr. Uday Kumar, an electrophysiologist who joined the fellowship in 2005 when it was in its infancy and helped to codify the learnings for future generations of fellows. His interactions with the administrative units at hospitals as well as health economics work led him to focus on applied and translational medicine with an emphasis on technology. He was exposed to the program during his fellowship at UCSF by way of interaction with Paul Yock, the program’s founder. He made steps to join the program as a fellow with the opportunity to focus on EP. Dr. Kumar credits the program for enabling him to gain exposure to the full life cycle of product development and with helping him identify and understand unmet needs, thanks to the consulting-like exposure to hands-on experience during the fellowship. This experience enabled him to launch iRhythm out of Biodesign and to help it grow to a current market capitalization of $1.5 billion, while helping over 400,000 patients to date with its patch technology capable of detecting heart arrhythmias. Though his experience was not the typical path, Dr. Kumar is an example of the type of individual these programs should hope to create — individuals who not only commercialize and launch a company to address an unmet need, but also continue to innovate. Dr. Kumar went on to found three more companies, most notably Element Science, which helps prevent sudden cardiac death by utilizing a wearable cardioverter defibrillator.18
Dr. Kumar’s experience was a personalized journey through purposeful steps while leveraging his domain expertise in EP. When Dr. Kumar joined the Biodesign Innovation Fellowship, he knew the issue concerning the detection of cardiac arrhythmias. The fellowship allowed him to bring together a team that was able to rapidly model and test its assumptions. Although many people doubted his team, it ended up receiving a provisional patent in 2006 thanks to the team members’ persistence. Further, the program allowed him to interact early with potential partners to demonstrate viability, enabling an initial funding round of $12.5 million in 2007. This funding allowed him to further recruit engineering expertise, such as Mark Day from Medtronic, to continue the growth of his company. Dr. Kumar’s success shows the opportunity multidisciplinary programs such as these provide to rapidly scale innovations.19
Strategy going forward
As the Stanford Biodesign program continues to evolve, Dr. Kumar and others want to focus on a number of things. Although people typically self-select into fellowships such as these, Dr. Kumar emphasized the importance of efforts to help target women and underrepresented minorities for entry into fellowship and leadership roles. The goal is to continue to recruit diverse participants to drive future success stories such as Dr. Kumar’s. Additionally, Dr. Kumar noted the change from OR-centric solutions to lower cost direct-to-consumer offerings. As a result, future solutions need to incorporate knowledge from not only mechanical engineers, but also electrical engineers and computer scientists, as the shift requires the development of a more robust spectrum of solutions. Moreover, to continue expanding the program, its supporters hope Stanford Biodesign can better partner with entities in the community to more effectively serve the population.20
Impact
Challenges and Growth of Programs across the Country
The challenges of Biodesign programs across the country revolve around time, mentorship and funding. Dr. Kumar highlighted the need to engage alumni to stay involved. However, matching appropriately skilled alumni who have time and are geographically close is difficult.21
Innovators in less established Biodesign programs, such as Dr. Francoise Marvel, a fellow in cardiology at Johns Hopkins who founded Corrie Health, had such troubles in finding mentors, resources and funding. Her startup was a digital health solution to help patients who have suffered from heart attacks manage their care. The idea came out of her intern experiences in cardiology service. Initially, she recruited talent to help her develop her product, by searching Hopkins for engineers and computer scientists via email blasts, class lectures and entrepreneurial interest groups. Even so, turning the idea into a reality took a significant amount of time. Dr. Marvel joined Hexcite, a product of the Technology Innovation Center at Hopkins for physicians launching digital health solutions, at its earliest stages. Although Hexcite connected her with the talent she needed and pulled her away from the physician dynamic to focus on innovation in a way similar to the fellowship at Stanford Biodesign, the most important aspects she emphasized were her intern elective experience, mentorships she sought out and a sense of genuine curiosity. Additionally, as Dr. Kumar attested to, every Biodesign program needs to focus on regional needs to succeed. Dr. Marvel received nondiluted funding from a Maryland Innovation grant to commercialize her product and promote job growth.22
Similar to the challenges Dr. Marvel faced at Hopkins in raising funds and finding time to further her venture, Massachusetts General Hospital faced issues through its Healthcare Transformation Lab (HTL). This program was launched in 2013 with grants from The Heart center. The goal was to create an innovation lab focused on emerging technologies and to introduce them to clinical delivery. Leaders at HTL, such Dr. Maulik Majmudar, a cardiologist and the associate director, realized that some of the difficulties physicians such as Dr. Marvel faced concerned having time and access to resources such as talent and industry leaders. Dr. Majmudar said HTL focused on three pillars: culture, deployment and evidence generation. These three pillars allowed innovators to work in an open-source and incubator-like environment while partnering with startups and testing their products at Mass General to gather data to drive clinical adoption. Dr. Majmudar also spoke about the issue of time, in particular, the Aetna Foundation Fellows Program that allowed two allied health professionals every year to have protected time to dive into their projects while receiving the cross-disciplinary tools for success (e.g., didactics from The Harvard Business School, public policy, and many other schools). This issue parallels the idea of Stanford’s Biodesign in the resources (e.g., design, engineering, law, medicine, business) that are given to innovators to train them for success in a multidisciplinary environment. Another challenge that Dr. Majmudar highlighted was finding the right talent and constantly pushing for the development of cross-disciplinary innovators. He hosts a monthly seminar open to all eight departments at the hospital to expose physicians to outside industries, such as AI/machine learning, entrepreneurship, licensing and legal, to connect them to outside hackathons, startup competitions and other leaders.23 This push to propel interactions across industries must be continually emphasized to effect meaningful change.
Whereas Biodesign groups such as Stanford’s Biodesign, Hopkins’ Hexcite and Mass General’s HTL have significant support structures for innovators, they are not the norm. Many such programs are in their infancy and lack centralized support for the training of cross-disciplinary innovators. Institutions such as Duke Health are hubs of great potential and innovation not just in the hospital, but also in the associated schools (e.g., engineering, computer science, policy, law and business), with many funding initiatives that provide great opportunities to launch and test innovations (Duke MedX, I&E, Discover and CTSA) but lack centralized groups to train these cross-disciplinary innovators to come up with ideas. Dr. Marat Fudim, a cardiology fellow at Duke Health, has taken up this issue within his department by creating didactics every quarter as a means of matchmaking between physicians and engineers. The idea behind this effort is to help physicians and engineers find potential solutions to problems or applications of their new technology. These ideas can then receive funding via internal departmental grants or from one of the other initiatives across Duke. The goal is to cross-train innovators through the sharing of ideas to find new and impactful solutions, similar to efforts at Stanford, Johns Hopkins and Mass General.24
Partnerships with outside stakeholders
One of the key successes of the Stanford Biodesign program was the early partnership with industry leaders. Johnson & Johnson and Abbott were early sponsors, and many corporate, VC and community partners have joined over the years. These types of partnerships are essential for any Biodesign program because they facilitate access to industry mentors, visits and externships for students, talent placement and general networking. Additionally, these sponsors donate to ensure the sustainability of programs such as Stanford Biodesign.25 All programs that want to create a Biodesign program should focus on partnerships with startups, industry leaders and corporate sponsors such as Aetna to build the network for participants to leverage.
Conclusion
LESSONS
The launch of the Stanford Biodesign program was a novel concept when Paul Yock initiated the Medical Device Network. However, since 1998, many similar programs have been launched to train these future cross-disciplinary innovators, not just in the cardiovascular space, but throughout medicine. Based on the research discussed above, there are five components required to support the growth of these innovative cross-disciplinary Biodesign programs. First, these programs need to establish formalized mentorship networks among both future alumni and industry leaders to allow participants to learn outside their areas of expertise from individuals with more varied practical experience, as seen through the mentors at Stanford Biodesign and MGH’s HTL. Second, didactics should be established to bring together individuals from varied backgrounds (e.g., medicine, engineering, business) to discuss the synergies in their skillsets to solve common problems, as seen at Stanford Biodesign, HTL and Duke Health’s cardiology department. Third, institutional grants and funding should be made available to help interested parties prototype potential solutions. Fourth, protected time via fellowships should be provided to help make these solutions a reality, as seen at HTL via the Aetna Foundation Fellowship and Stanford Biodesign via the Innovation Fellowship. Fifth, programs should also focus on geographic needs; as Dr. Kumar mentioned, local partnerships, funding and talent can be acquired to enable success.
Short- and Long-term implications FOR cardiovascular health
Stanford Biodesign initially focused on cardiovascular health, because many early applications concerned stents and balloon angioplasty. Similarly, Mass Generals HTL focused on cardiovascular health in its first two years but quickly expanded its scope. These programs started in cardiovascular health because of the significant crossover between technology and cardiology, and many more such programs may start out this way. As programs such as these proliferate throughout the country, innovations in cardiovascular health will grow rapidly in the near future. This growth will lead to new advancements that cardiologists will have to be trained to use. These advancements, although positive in nature, will lead to short-term disruptions in the cardiologist’s workflow, as was the case with the rapid consolidation of individual cardiology practices into larger systems. Thus, as these innovations continue to be developed, integration must be kept top of mind to ease their use. Furthermore, as these ideas continue to flow, distilling the truly disruptive ideas from the toys that provide no meaningful value to the patient is vital.26
As for long-term implications, these programs will expand to other service lines; thus, the paradigms will shift within cardiovascular health at an even more fevered pace. However, to stay focused, programs such as the ones at Stanford and Massachusetts General, as well as events such as the Cardiovascular Innovation Summit, need to provide guidance focused on the specific needs that innovation can solve, and to provide engagement with cross-disciplinary experts.27 Many programs such as Stanford Biodesign already provide this guidance to ensure innovations in the long term solve key unmet needs; however, other programs must follow suit.
A final long-term implication is that although many solutions in cardiology may be easily implementable, such as cardiac monitoring and biostents, many others, such as the use of genetic biomarkers to identify susceptibility to certain cardiovascular diseases, may be cost prohibitive or not demonstrated to affect patient outcomes; thus, caution must be taken as innovations are incorporated into the workflow. Furthermore, new innovations may simply be so complex that the period of adoption may be long and therefore require patience. For example, procedures in robotic surgeries in cardiac revascularization and valve surgery are long, require extensive training and have a high learning curve. Therefore, adoption is slow despite the clear benefits to the patient.28
These innovations will continue to permeate through the cardiovascular space for both the short and long term as cross-disciplinary innovators find unique solutions to difficult problems. Identifying the truly disruptive innovations and thoughtfully integrating them into the workflow with patience and caution is therefore important.
Endnotes
- “Innovation in Healthcare: Why It’s Needed and Where It’s Going,“ Health Catalyst. https://www.healthcatalyst.com/the-rising-healthcare-revolution-the-future-is-already-here/
- D.B. Duong et al., “A Model for Training Medical Student Innovators: The Harvard Medical School Center for Primary Care Abundance of Agents Change Program,“ Med Educ Online 21 (2016): 30662. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4910306/
- “Physician Innovation Network,“ AMA. https://innovationmatch.ama-assn.org/
- R. Thomas, “NYU Hosts First-Ever Healthcare Makerthon,“ Entrepreneurial Institute (2015). http://entrepreneur.nyu.edu/blog/2015/11/19/new-york-university-hosts-first-ever-healthcare-innovation- makerthon/
- Bora Chang, phone interview by Sanjit Misra, May 8, 2018.
- “About the Cardiovascular Innovation Institute,“ Cardiovascular Innovation Institute. https://cv2i.org/about- cii/
- “Multidisciplinary Cardiovascular Research Training,“ Michigan Medicine, Center for Healthcare Outcomes & Policy. https://medicine.umich.edu/dept/chop/training-education/multidisciplinary-cardiovascular-research- training
- “About Us,“ Center for Health Technology & Innovation (CHTI). https://ahahealthtech.org/about-us/
- “About,“ Health2047. https://health2047.com/about/
- “Healthbox Empowers Innovation Strategies,“ Healthbox. https://healthbox.com/about-us
- “Join,“ MATTER. https://matter.health/join/
- “About Us,“ Synecor. http://synecor.com/about-us/
- B. Knapp et al. “Ten Simple Rules for a Successful Cross-Disciplinary Collaboration,“ PLoS Computational Biology 11, no. 4 (2015): e1004214. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4415777/
- “Timeline & History,“ Stanford Byers Center for Biodesign. http://biodesign.stanford.edu/about- us/timeline.html
- “Vision & Mission,“ Stanford Byers Center for Biodesign. http://biodesign.stanford.edu/about-us/vision- mission.html
- “Our Process,“ Stanford Byers Center for Biodesign. http://biodesign.stanford.edu/about-us/process.html
- Lyn Denend, phone interview by Sanjit Misra, March 29, 2018.
- Uday Kumar, phone interview by Sanjit Misra, April 2, 2018.
- “iRhythm Panel,“ Biodesign Alumni (2017). https://biodesignalumni.com/2017/08/06/irhythm-panel/
- Uday Kumar, phone interview by Sanjit Misra, April 2, 2018.
- Ibid.
- Francoise Marvel, phone interview by Sanjit Misra, March 15, 2018.
- Maulik Majmudar, phone interview by Sanjit Misra, April 2, 2018.
- Marat Fudim, phone interview by Sanjit Misra, April 5, 2018.
- “Industry Sponsors,“ Stanford Byers Center for Biodesign. http://biodesign.stanford.edu/giving/industry- sponsors.html
- B. Schallhorn, “Challenges and Change Management in Cardiac Technology Innovation,“ Diagnostic and Interventional Cardiology (2014). https://www.dicardiology.com/article/challenges-and-change- management-cardiac-technology-innovation/
- “Cardiovascular Innovation: Moving Cardiovascular Care Forward Summit,“ Cardiology Magazine, American College of Cardiology (2016). http://www.acc.org/latest-in- cardiology/articles/2016/11/29/10/39/cardiovascular-innovation-moving-cardiovascular-care-forward/
- “Innovation and Cardiology: The Future is Now,“ Cardiology Magazine, American College of Cardiology (2016).
http://www.acc.org/latest-in-cardiology/articles/2011/09/27/09/41/innovation-and-cardiolgy-julaug2012/
-
-
Driving Innovation
-
Innovations in Cardiovascular Health
-
The Role of Physicians in Driving Innovation
-
The Role of Patient Groups in Driving Innovation
-
Clinical Innovations in Cardiovascular Health
-
What Drives Innovation in CV Health?
-
The Rise of Academic and Contract Research Orgs
-
Federal Regulations as Accelerators
-
Reimbursement Models
-
Consumer Technology
-
Training Cross-Disciplinary Innovators
-
Conclusion